
An Attempted Defence of Functionalism Against the Cross-wired Brain Thought Experiment
Published:
I wrote this final essay for the PHIL407 Philosophy of Mind I course I took during the Fall 2021 semester. I had been waiting patiently for this course to fit in my course schedule so that I could take it, and I did not hesitate one bit from taking it when I noticed that it clashed with none of my courses at the beginning of my course. It was one of the best decisions of my undergraduate education (I was still continuing my maths double major, so I was still an undergrad), and I did continue to take the second course PHIL408. There is also a short version that I wrote as a submission to SCSS2022, but sadly I wasn’t accepted.
1. Introduction
The functionalist conception of the human mind models it as a set of states characterized by causal roles, where each state can be caused by sensations and cause behaviour, as well as play a causal role in the activation of other states (Kim, 2011). The cross-wired brain thought experiment challenges functionalism by claiming it fails to account for the qualia of mental processes: A patient, with both the inputs and outputs to, say, the itch and pain subunits of their brain switched, would behave appropriately upon relative input but supposedly would experience the qualia of the wrong phenomenon. In this essay, I offer a way out of this challenge within the functionalist framework. Firstly in Section 2, I present the thought experiment and take a close look at the methodological aspects, then expose the faults in the line of thinking of the experiment. In Section 3 I present my solution to the challenge posed by the experiment, with its properties and their motivations. Finally, in Section 4, I summarize my ideas and criticize them myself.
2. The Experiment
2.1. The Crazy Neurosurgeon
I take the thought experiment as it is presented by Kim (2011). The story goes as follows: Suppose I am abducted in my sleep by a crazy neurosurgeon who wishes to perform a complex and sinister operation on my brain. The neurosurgeon is an expert of all neural circuitry in the brain, able to localize any sort of neural circuitry that implement various aspects of human psychology, in this case, the pain and itch sensations. The neurosurgeon identifies the neural circuits that implement these two operations and switches both their inputs and outputs and they proceed to patch me up perfectly fine with my newly rewired brain and relocate me to my bed.
Before we proceed further, let’s take a look at some crude schematics of the relevant neural circuitry of my brain, as shown in Figure 1. Originally, the relative sensory inputs go to their relative neural circuits and through their computations cause appropriate behavioural output, as depicted in Figure 1 (left). After the operation because both the inputs and the outputs are crossed as shown in Figure 1 (right). The inputs cause the wrong neural circuit to activate, but these activations still cause appropriate behaviour.1 From here on, I will use the terms neural circuits that implement various functional states as boxes for simplicity just like Kim: The pain receptors trigger the Pain Box which produces pain behaviour, and vice versa. The terms “neural circuit” and “box” wil be used interchangeably.
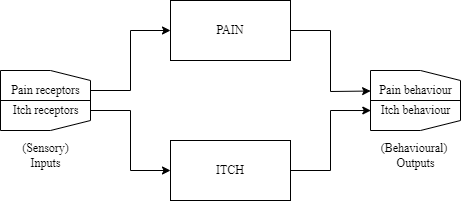
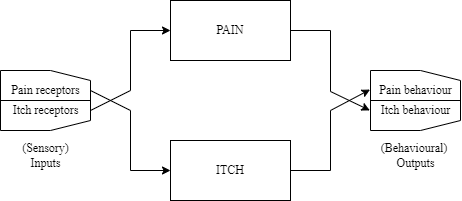
Figure 1: Crude schematics of my brain's relevant parts, pre-operation (left) and post-operation (right).
Now, what happens when I wake up in the morning and hit my pinky toe to the side of my bed frame? Following the schematic in Figure 1 (right), I would act appropriately on the outside: Most likely curse and start jumping on one leg. How about on the inside? What would be my subjective experience with my post-operation brain?
This is the main point of challenge for the thought experiment, as it creates a version of the inverted qualia problem (Kim, 2011). Prima facie, one would say that I would be experiencing the itchiness of an itch when I hit my pink toe, and conversely that I would experience the painfulness of a pain when my friend pranks me with itch powder. Functionalism seems to fail to give a satisfactory account for such an inversion of qualia or even (in an other line of thinking) lack thereof.
2.2. The Neurosurgeon’s Methodology
On a tangent, let’s take a closer look at how the neurosurgeon’s method during the operation. At first glance, we may believe that the neurosurgeon would follow the causal chain forwards from the inputs on: Trace the pain receptors and the intermediary neurons they trigger, and the neurons that they trigger and so on. It is clear that such a tracing would be fruitless. Even if the neurosurgeon encounters the neural circuitry that implements, say, the pain mental state and eventually its output behaviour, they would be unable to isolate them from other neural circuitry dur to the immense connectivity of the human brain. The result of such a forward causal tracing would most likely yield a significant portion of the human brain as these neurons have the potential to trigger many other neurons, most of which most likely not significantly relevant to pain (or any other function we are interested in), if at all. So, asking “Which neurons can these pain receptors eventually fire?” is not sufficient in determining the neural circuitry that is the Pain Box. Let’s call this first question as Q1.
What may be a solution to this? I say the neurosurgeon must follow a second, backwards causal route as well. Starting from the outputs, which are the appropriate motor neurons, the neurosurgeon follows the causal network (on its implementation, that is) in the backwards direction. This analysis yields all the neural circuitry that has the potential to cause such behaviour, so the question this time becomes “Which neurons can eventually cause these motor neurons to fire?” Let’s call this question Q2. Similarly to the forwards tracing case, this analysis would point to an immensely large section of the human nervous system. But this time, the neurosurgeon also has the forwards tracing data. Intersecting the two sets of neurons yielded by the two questions and effectively asking “Which neurons fire due to the firing of these pain receptors and cause these motor neurons to ire?”, the candidate neurons would be to those linking the pain receptors to the lying on a directed path from the appropriate inputs, to the appropriate output, reducing their numbers.
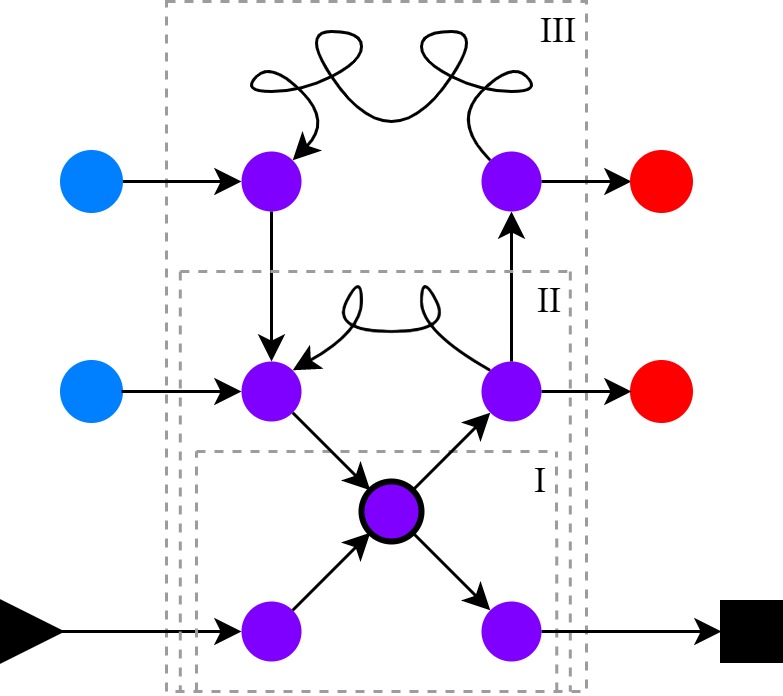
Figure 2: A sample neural network, with arrows indicating causation of firing. The triangle is an input neuron (e.g. firing of pain receptors), the square is an output neuron (e.g. firing of motor neurons), and the disks are intermediary neurons. The curved arrows indicate long causal links through several states.
Is the combination of these two questions enough? Let us play the role of the neurosurgeon with the sample neural network given in Figure 2 to discover the neural circuitry (the box) of a certain function that occurs upon the activation of the triangle neurons and ends with the activation of the neurons (representing behaviour) indicated by the square neurons. The intersection of the answers to Q1 and Q2 give us the purple intermediary neurons, but the question as to which of those are essential in describing the phenomenon remains. There appears two be three choices of neural circuitry indicated with roman numerals on the figure: One directly through the three neurons without any loop (I), one with a relatively short loop (II), and one with a long loop (III). Which one should we go for to identify the “box” we are looking for?
The point of this example is to illustrate that some kind of minimality must be employed when determining the causal implementation of a given psychological function, as one can find arbitrarily length causal chains that link the inputs to the outputs. This does not mean that the shortest one is the ideal one, however. Processes or functions may necessitate such loops: For example although loop II may contain some irrelevant neurons, the non-looping direct pathway may be too simplistic for an apt description of the function we wish to describe, so we would opt for the trajectory of loop II. It is up to the neuroscience/psychology to figure out these restrictions.
As a final note on the neurosurgeon’s method: One may find this starting-from-nothing approach of the neurosurgeon described so far quite odd. Surely, such a crazy genius would know of the rough location of the pain center and the sensorimotor cortex in the human brains. Why would they start from nothing to discover what is what and is not? This is true; however, the crucial point is that even if the neurosurgeon themself need not follow such a procedure, neuroscience must have followed it prior the operation. The neurosurgeon simply accesses that body of knowledge to bypass the whole discovery procedure so they do not reinvent the wheel, which does not invalidate the current argument.
2.3. Objections
I will present multiple objections, which are seemingly different but take root in the same principle: The privacy of mental experiences (PME). The principle states that only the bearer of the mental states has direct access to their own mentality. In the narrative of the thought experiment as it is presented, only I, the victim of the neurosurgeon, have the epistemic privilege of accessing my own experiences.
Empathetic Projection: The experiment as-is seems to be working because we are falsely attributing qualia to the patient via empathy in the most general sense. The data from which we infer the others’ mental states is nothing other than the observed behaviour due to PME. We fill in the causal gap between the inputs to the other person and the observed output behaviours based on what we would do and, more importantly, how we would feel. But necessarily, any such simulation or inference is run through our own non-operated2 brains. Our internal model has a fundamental mismatch with the patient, so any such attribution is at best unfounded or at least arbitrary. On this front, the experiment works by appealing to our common sense, which is hardly a solid base for scientific induction.
Scientific Hammerhead and Ghost of the Neurosurgeon: If we are not going to trust our own mental models to assess the mental experiences of the patient, perhaps we could refer to the neurosurgeon (or neuroscience in general). In the end, they are the one who made the switch between the two boxes, they should also have some credibility on the reflections of this operation on the patient. Could the neurosurgeon, perhaps, “science” their way into discovering the mental experience of the patient? This brings me back to the neurosurgeon’s methodology as examined in Section 2.2. The minimality employed by the neurosurgeon pushes them to isolate the neural circuitry that makes the patient disposed to act in accordance with the relevant input. Because again, the only data we have is the patient’s (or in general humans’) observed behaviours upon various stimuli, which excludes any neural circuitry that does not directly contribute to putting the patient in the correct dispositions out of the box that the neurosurgeon is trying to identify. This way, the circuitry that implements the qualitative aspects of a certain mental event is left out of the box during the identification process, as they are (almost by definition) immune to discovery by observing behaviour.
On a similar vein, the neurosurgeon’s (questionable) right to assess the mental state of the patient (one beyond our usual, external observations) disappears after the patient is patched up. Nobody aside from the patient observes the mental state of the patient to make claims such as “This neural circuitry is firing quite well, so the patient is experiencing pain.” In other words, a ghost of the neurosurgeon does not remain in the patient’s brain to make such claims.
3. The Qualia Box
While being faulty in its conclusions, the cross-brain thought experiment illustrates the following fact quite vividly: We do not know the qualitative experience of the patient because they act just like before, even though there has been a change in the physical implementation of their mentality. It is also clear that we have come to a distinction between being disposed to act in a certain way, and experiencing the qualitative aspects of the mental events. These two aspects of the same mental event are naturally tightly correlated, but this does not necessitate they be implemented within the same mental state.
I claim that separating the two into two different kinds of states, one containing the dispositional aspects and the other the qualitative ones, provides a solution to this challenge within the functionalist framework. This separation is motivated by the neurosurgeon’s methodology, as they seem unable to discover the qualitative aspects during their process of identifying the pain and Itch Boxes. So, let us clump together all the qualitative aspects of mental phenomena into a single box and call it the “Qualia Box”. For the sake of simplicity, I will take it here as a single state implemented by a single box, but one could extend it to be multiple interacting states. We can take the Qualia Box as the “mind’s eye” of the patient that observes the mental going-ons of the patient. It observes the dispositional boxes, regulates them when needed, observes itself and modifies itself when needed.
In the rest of my essay, I will first be handling the thought experiment with this updated model to first make an exposition of my line of thinking and to hopefully convince the reader that it serves this purpose well. Then, I will be discussing the properties of this Qualia Box, try to justify them and give examples that support my claims whenever possible.
3.1. The Crazy Neurosurgeon Strikes Back
Let us go through the thought experiment once more. I am abducted by the neurosurgeon, who wishes to make an operation on me. Before the operation, the crude diagram of my relevant mentality is given in Figure 3. During the operation, the neurosurgeon can only discover the dispositional states because the only available evidence to discover any mental state can only be behaviour, and the neurosurgeon has to employ a minimalistic approach when identifying each box. So, the neurosurgeon finds the pain disposition and itch disposition boxes. Therefore, during the operation, the neurosurgeon unintentionally switches the connections to the Qualia Box as well, to obtain the rewiring in Figure 3.
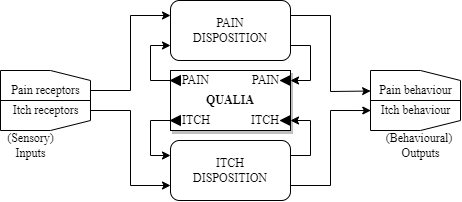
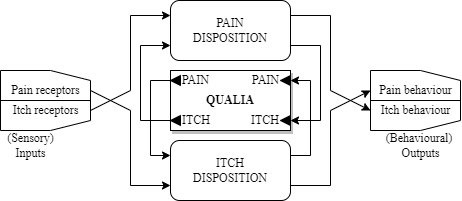
Figure 1: Figure 3: Updated crude schematics of my brain's relevant parts, pre-operation (left) and post-operation (right).
Now, let us again ask the question: What happens the morning after, when I hit my pinky toe to the side of my bed frame? Here is the chain of causation: My pain receptors activate the itch disposition box, which trigger the pain behaviour on the output side. So, no changes here. On the other hand, the itch disposition box goes and triggers the pain input of the Qualia Box, so the mind’s eye observes what is happening to be pain, and modifies it accordingly through the pain output of the Qualia Box. I am, then, experiencing the appropriate qualia associated to the event!
3.2. Properties & Motivation
Before we go on with the properties of the Qualia Box, let us first discuss how we would define it. The Qualia Box is responsible for containing the mental representations of other mental states, including itself. The Qualia Box cannot take input from the outside, it pieces together what outside may be through the contents of the dispositional mental states. It can therefore be considered as the seat of consciousness. This line of thinking is very much in line with the ideas of Hofstadter (1999). He describes human mentality as a set of “tangled hierarchy” of symbols, and the symbol for self is an overseeing symbol that communicates with all the others, even with itself. He describes the actions and properties of such a symbol as follows:
… [T]his way of describing awareness-as the monitoring of brain activity by a subsystem of the brain itself- seems to resemble the nearly indescribable sensation which we all know and call “consciousness.” Certainly one can see that the complexity here is enough that many unexpected effects could be created. For instance, it is quite plausible that a computer program with this kind of structure would make statements about itself which would have a great deal of resemblance to statements which people commonly make about themselves. This includes insisting that it has free will, that it is not explicable as a “sum of its parts”, and so on. —Hofstadter (1999) Chapter XII, Minds and Thoughts, p.388
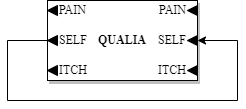
Figure 4: The Qualia Box. The self-connection was omitted for clarity in the previous schematics.
Recursivity and Chaotic Behaviour. Figure 4 shows the Qualia Box in one more additional detail, which is the self-connection. This makes the Qualia Box create and contain representations of itself3, falling in line with our self-observing mental eye phenomenon. It also comes with its own set of restrictions: It would be sensible of us to require this system, be it modelled in discrete-time or continuous-time, to possess some sort of stability property, at least within reasonable time windows. Otherwise, it may not even be sensible to talk about such a representation. On the other hand, if we are ever going to model such a system scientifically, it will be a mathematical model, and even the simplest of mathematical models can exhibit chaotic behaviour (May, 2004). This chaotic behaviour puts our everyday predictability assumptions away as explored by Lorenz (1979) in a different model to May. Therefore I find it reasonable, and further explanatory, to take this causal structure to be chaotic. Chaotic nature of the Qualia Box would explain the inexplicable nature of qualia as well: It would, first of all, render any knowledge of the causal rules of the Qualia Box essentially useless in predicting or simulating the qualia of phenomena, as even the slightest difference in the simulation (which are most probably quite frequent and not very slight) will render the simulation powerless in predicting the outcome.
Inaccuracy in Representations. Our qualitative experiences are shaped by the dispositional status and themselves constantly, without us noticing them. One very simple example of this is the blind spot we have in our vision (AsapSCIENCE, 2016). The illusion is due tp the entry point of the optic nerve to the eyeball, where there is no optic receptor to perceive light, creating a sizeable blind spot in our visual stream. The experiment reveals this blind spot, and even then it does not appear as a literal blind spot, but as an obviously faulty visual experience interpolated by the surrounding visual data. To me, this experiment/illusion points to the obvious fact that our own experience, be it dispositional or qualitative, is constantly modified. The recursivity of this reconstruction is due to the interpolation made on the patch: The cognitive processes are clearly making use of the current or past inputs to create the visual experience.
Situatedness. Finally, all of the claims explained so far put consciousness and cognition in a situated framework. Knowing the properties of the physical structure and the rules of causation between the physical states corresponding to causal-functional states becomes insufficient in explaining the mental experience of a subject in present because no matter how precise our measurements are, there will always be a margin of error, within which the sensitive chaotic model can take on to depict completely different behaviours. This deterministic-yet-unpredictable nature of a mental model essentially implies that properties of a subject pertaining to cognition and/or consciousness are unique to those physical conditions. Mental event types can nonetheless be characterized by their causal-functional descriptions, i.e. the causal roles they play within the causal net of a psychological theory, but mental event tokens are specific in space and time.
4. Conclusion
After the examination of the thought experiment and the attempted solution to the challenge it poses so far, let us go back to the difficulties functionalism faces more concretely in the face of the cross-wired brain experiment, or more generally, the qualia inversion argument. By separating dispositional aspects from qualitative aspects, this new functional perspective has the power to counter both the qualia inversion and even the absent qualia arguments: In the qualia inversion case, the dispositional states are left intact and the qualitative ones are rearranged4. In the absent qualia case, we omit the Qualia Box from the picture. While this may be easy to say, it likely necessitates some more changes on the dispositional states as they would have to implement the changes to the dispositions the Qualia Box would have made without actually coming to possess its properties (recursivity, chaotic nature, etc.). We make the classification into dispositional and qualitative based on the properties of the states at hand, not just because we name/wish them to be. The reader can think of the difference between the recursive and non-recursive implementations of the factorial function as an excessively simple example for such a difference.
On the other hand, I realize the argumentation I have made so far is not bulletproof. For example, the neurosurgeon’s minimality criterion is left as vague as possible. How can the neurosurgeon come to decide which neurons (or functional atomic elements of the implementation in question, e.g. set of logic gates on a microprocessor) belong to the box? There is also no guarantee that the qualitative states would remain outside the said box even with a valid minimality criterion. On the other hand, in the last paragraph of Section 2.2, I mention how the neurosurgeon loses any right to assess the mental state of the patient after they are patched up. Let us imagine a future where we have the ability to measure each and every single neuron in real-time and in vivo on an accurate anatomical model of the nervous system. This way the neurosurgeon would still be able to trace the neural pathways of the patient with no need for an operation, and the activation of the neurons in various situation. Can the genius neurosurgeon still judge the mental state of the patient, together with the qualitative aspects? The (presumably) chaotic nature of the qualitative neural circuits prevent us from predicting any future state, but does this imply we cannot judge the present state with real-time measurements? These are a few of the questions that are left unanswered in this essay, and I have no doubt the reader can come up with more.
Nonetheless, I hope I could convince the reader that the separation of a mental state into two states, dispositional and qualitative, serves to counter the challenge the cross-brain thought experiment poses. While it may be unsettling to see the familiar and indescribable feeling we have of our mental events laid out with such transparency and in mechanistic terms, if true, it will be a truth we have to face.
Notes
- One might object by questioning how such a criss-crossing is even possible, how either box does not go haywire to produce nonsensical outputs. On the other hand, the figure depicts the two behaviours to be different outputs, whereas they could be the activation of the same physical system, such as the retraction of the hand when it is cut (pain) or when it is stung by a stinging needle (itch). I will not be dealing with such details. Although I suspect they could serve for other meaningful bases for objection, these would not be relevant to my current objections. Back up.
- Hopefully, at least. Back up.
- This representation would contain and be a representation of itself, which is in turn a representation of… Back up.
- One may here object to such a rearrangement by claiming it is impossible, as the qualitative states are tangled with the dispositional ones and such a rearrangement may not even make sense or “compute.” Well, if the reader was comfortable so far with the possibility of interchanging the dispositional states, or even the criss-crossing in the original thought experiment, I see no reason why they cannot be comfortable with this rearrangement as well. If the reader was uncomfortable with those as well, I don’t see how they could have read so far and not object to the original thought experiment to begin with. Back up.
References
AsapSCIENCE. (2016). You can’t see this (mind tricks). YouTube. Retrieved from https://www.youtube.com/watch?v=0NPH_udOOek
Hofstadter, D. (1999). Gödel, Escher, Bach: An Eternal Golden Braid. Basic Books.
Kim, J. (2011). Philosophy of Mind. Westview Press.
Lorenz, E. (1979). Predictability: Does the Flap of a Butterfly Wings in Brazil Set off a Tornado in Texas? Proceedings American Association for the Advancement of Science in Washington.
May, R. M. (2004). Simple Mathematical Models with Very Complicated Dynamics, 85–93. Retrieved from https://doi.org/10.1007/978-0-387-21830-4_7 doi: 10.1007/978-0-387-21830-4_7
Short version
(Back up to the longer version)
The cross-wired brain thought experiment challenges functionalism by claiming it fails to account for the qualia of mental processes: A patient, with both the inputs and outputs to, say, the itch and pain subunits of their brain switched, would behave appropriately upon relative input but supposedly would experience the qualia of the wrong phenomenon.
The experiment as-is seems to be working because we are falsely attributing qualia to the patient, e.g. based on empathy, when the only authority on such claims can be the patient. While we believe the dispositional and qualitative aspects of a mental state may reside in a single state, splitting them into two causally interacting yet different mental states solves the problem. The qualitative states are responsible for the quale of phenomena, while the dispositional states are directly responsible for producing behaviour. The two kinds of mental states causally interact, but the qualitative states can only influence behaviour through their dispositional counterparts. Then, the neurosurgeon would be unable to figure out the implementations of the qualitative states within the causal structure via experimentation, as such qualitative states are behaviourally undiscoverable. Therefore, the neurosurgeon would unknowingly switch the qualitative states during the operation. The patient would experience the appropriate qualia post-operation, the difference being the implementations of the pain and itch dispositional states.
This distinction between dispositional and qualitative mental states explains various observations. The claim that qualitative states have causal effects on their dispositional counterparts can explain visual illusions, e.g. the blind spot in our visual stream due to the lack of photoreceptors on the entry point of the optic nerve to the eye. While we may discover this blind spot through experimentation, we never realize it ourselves, pointing towards a modification of the visual inputs to produce our experiences and dispositions in visual judgements. This causal power on the dispositional states implies recursive causation between the dispositional and qualitative states, which can explain the inexplicable nature of qualia given that the process is chaotic, rendering it unpredictable yet deterministic.
This approach suggests a difference between mental states/qualia in general and their implementations in a particular physical system. The causal rules describing the qualitative state is shared across implementations, but any difference in physical conditions leads to unpredictable/inexplicable behaviour. Knowing the causal mechanism producing qualia is insufficient to predict its physical realizations because of the process’s sensitive dependence on initial conditions, i.e. its chaotic nature.